Anaemia and the Copper-Deficient Patient
InterClinical eNews November 2018, Issue 86
Copper deficiency is a less common and under-recognised cause of anaemia, producing an anaemia unresponsive to iron, vitamin B12 or folate. In this journal article four expert reviewers highlight the key features, the likely causes, the populations affected and how to treat the symptoms.
Copper Deficiency Symptoms
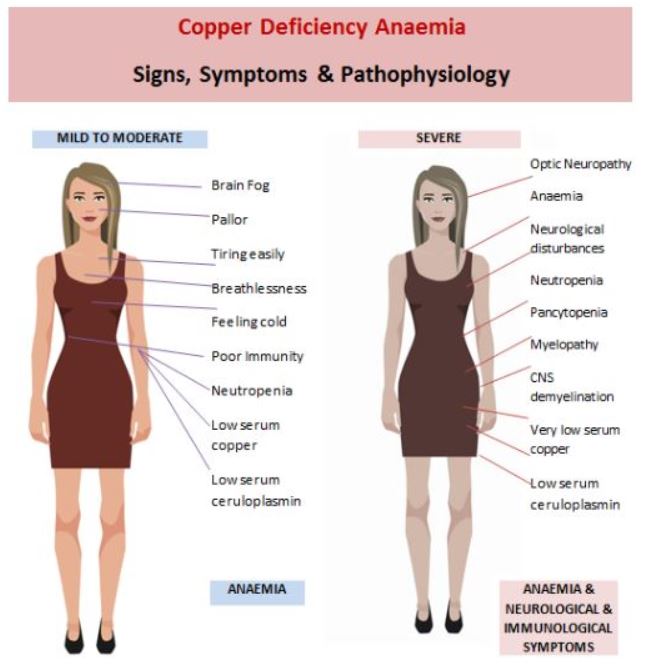
Mild copper deficiency is largely indistinguishable from other types of anaemia, apart from a persistent neutropenia. As it progresses in severity the symptom picture becomes more complex and neurological and immunological symptoms manifest. The main symptoms of mild and severe stages are outlined in the diagram below:
Time until Diagnosis
This review points to a long gap between the onset of anaemic symptoms and a diagnosis of copper deficiency. Early diagnosis happens rarely, in fact, copper deficiency is not usually diagnosed until a year after symptoms present. At first, it can appear as a simple anaemia, but over time the symptoms develop to present a much more complex picture.
Conditions that Mimic Copper Deficiency
Mild to moderate copper deficiency may be mistaken for several other types of anaemia such as iron or folate. As neurological symptoms develop it begins to mimic vitamin B12 deficiency. As it progresses, a severe deficiency can mimic other conditions such as myelodysplastic syndrome due to commonly observed abnormalities in bone marrow. These abnormalities may include vacuoles in myeloid precursors, iron-saturated plasma cells, a reduction in granulocyte precursors and ring sideroblasts. Cytogenetic studies are needed to rule this possibility out.
At-Risk Populations
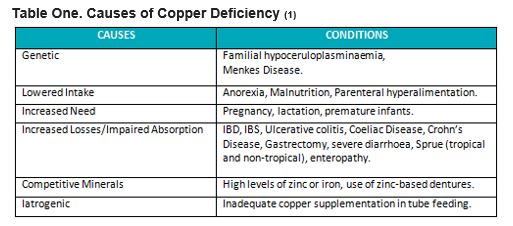
The main causes of copper deficiency are outlined in Table 1. The most common causes of copper deficiency are either hereditary or acquired.
Early Diagnosis Important
The review highlights that although mild to moderate copper-deficiency haematological symptoms appear to be completely reversible, severe deficiency symptoms such as neurological issues are only partially reversible. These neurological conditions can include myeloneuropathy, gait disturbances, motor neurone disease, spasticity, and CNS demyelination. Thus, severe deficiencies usually leave some residual permanent neurological damage.
Treatment Options
The authors recommend oral ingestion of 2 mg of copper per day for mild to moderate copper deficiency, whereas a severe deficiency may require copper infusions followed by oral ingestion of 3 – 8 mg per day until levels return to normal. HTMA is a good indicator of copper status in the body.
INTERCLINICAL COMMENT
It is important to rule out copper deficiency as a cause of unresponsive anaemia since, in addition to the debilitating symptoms of anaemia, it can lead to irreversible neurological damage if not discovered and resolved early enough.
REFERENCES
- Myint ZW, Oo TH, Thein KZ, Tun AM, Saeed H. Copper deficiency anemia. Annals of hematology. 2018 Jun 29:18.
Copyright InterClinical Laboratories 2018, 2020
No Comments
Sorry, the comment form is closed at this time.